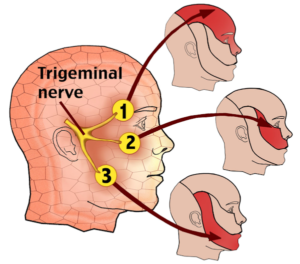
Trigeminal Neuropathy (V Cranial Nerve)
Trigeminal injury is the second more frequently described feature among cranial neuritis in SS patients; in fact, trigeminal neuropathy was observed in 102/267 (38%) cases, isolated or associated with other cranial nerve involvement.
Involvement of IX, X, XI, and XII Cranial Nerves
A few reports described SS patients who presented difficulty of swallowing, which is a symptom of glossopharyngeal neuropathy ; this nerve involvement was always reported in cases of multineuritis. All cases seem to be related to transient, often recurrent episodes of multineuritis, generally responsive to treatment.
Neurologic Complications Associated with Sjögren's Disease
Trigeminal neuralgia (TGN) is characterised by sudden severe brief episodes of recurrent stabbing pain in the distribution of one or more branches of the fifth cranial nerve. It is relatively rare and the majority of cases present unilaterally.
Symptoms of TGN include jaw pain that may be aggravated by chewing, swallowing, talking, touch,or by consuming hot or cold food and drink.
The pain can be triggered by shaving or wind blowing across the face.
The severe paroxysms of pain are often described as ‘shooting’, ‘sharp’ or ‘electric’.
An attack has rapid onset and lasts between 10 seconds and a couple of minutes, followed by a refractory period.
The generally accepted common cause is compression of the Gasserian ganglion (sensory ganglion of the trigeminal nerve) or its branches by a blood vessel.